
Environmental determinants of disease
Introduction
The environment may be taken to encompass all external factors and conditions that affect people’s lives. From a health perspective, the definition may be wide and include social factors, but often it is taken to have a more restricted meaning of the chemical, biological and physical agents that impinge on health. Traditionally, the focus of public health work has been concerned with local health hazards – pollution of the air, water, land etc – but in recent years there has been growing concern with a number of global hazards such as stratospheric ozone depletion and climate change. The types of environmental influence that populations suffer (and give rise to) are broadly related to their socio-economic development. They are also inequitably distributed. Recent estimates of the global burdens of disease from environmental factors shows that the greatest burdens relate to unsafe drinking water, poor sanitation & hygiene, and to pollution of the indoor and outdoor air. Burdens relating to climate change, which currently are modest, are expected to increase substantially over time.
Key definitions and terms
|
DALYs |
Disability adjusted life years: the sum of the years of life lost due to premature mortality (YLL) in the population and the years lost due to disability (YLD) for incident cases of the health condition. |
|
Environment |
The surroundings and external conditions, especially as affecting human lives. |
|
Environmental justice (EJ) |
The notion of equity and justice in relation to environmental exposures and related health burdens born by groups defined on the basis of such factors as socio-economic status, ethnicity and gender. |
Environment and health
|
Definitions |
Last (Dictionary of Epidemiology, OUP[1]) defines the environment as 'all that is external to the human host'. It can be taken to include anything except genetic factors, but is usually thought of as including physico-chemical, biological, social and cultural factors, which individually and in combination influence human health and well-being. The following notes concentrate on the physical, chemical and biological environment, and give less emphasis to broader socio-economic influences. |
|
Environmental justice |
It is important to note however that socio-economic factors lie behind many of the large differentials in health within populations and between them. In relation to the environment, socio-economic deprivation is important as a frequent determinant of environmental exposures (on average poorer people tend to live in more polluted, less healthy areas) and are more vulnerable to the effects of such exposures by virtue of their health status and poorer access to services. At the same time, people in more deprived areas, who tend to consume fewer resources, are typically responsible for fewer of the emissions that cause environmental contamination. This is often labelled the issue of environmental justice (or injustice). Examples of inequities in exposure and health effects can be found in relation to many environmental factors. Examples include:
|
|
Trends in environment and health concerns |
Until the 1980s, environment and health concerns were often focused on the adverse consequences for health of the increasing release of chemical contaminants into local environments, and on exposures related to industrialisation and urbanisation. Particular concerns arose in relation to outdoor air pollution, contamination of water bodies and the land, and radiation risks. These concerns often received prominence with serious pollution episodes, some examples of which are:
The occurrence of key environmental incidents and accidents raise public concern and often lead to new trends in research and interest on the effect of the environment on health. |
|
Industrialisation and urbanisation |
Industrial development and urbanisation has been a major and continuing global trend. Half of all people now live in urban environments, and urban life is often polluted and unhealthy, especially in low income countries. Large cities in poorer countries typically combine the environmental problems of poverty with those of uncontrolled urban expansion, squatter settlements and unregulated industrialisation. Residents therefore often face the combined hazards of poor sanitation, unsafe drinking water, precarious housing, dangerous roadways, polluted ambient and indoor air, and toxic wastes. |
|
Global environmental change |
In recent years, it has increasingly been recognised that human activity is now giving rise to a set of large-scale environmental problems, with capacity to cause adverse effects at a global scale. Such activity is reducing biodiversity at an unprecedented speed, depleting non-replenishable resources, and altering the gaseous composition of the lower and middle atmosphere. Among the more prominent effects with potential bearing on human health are:
Global change should be distinguished from globalisation, which refers to the processes that lead to increasing flows of people, goods, information and ideas across the world. Globalisation is itself an important influence on health because of its bearing on such factors as the spread of (transmissible) disease, the export from high to lower income countries of occupational exposures, and the economic factors that contribute to health inequalities and unhealthy patterns of production and consumption. |
Relationship of environmental risks with development
|
Kuznets curve |
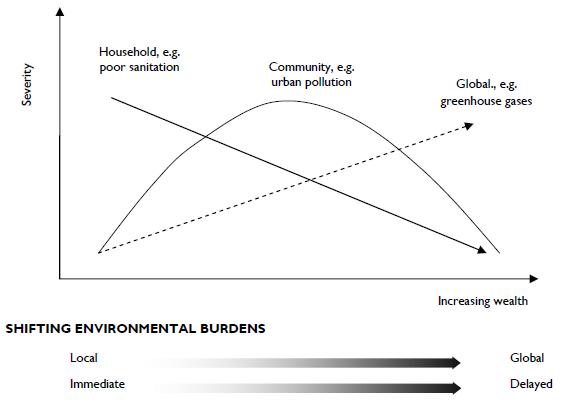
For many environmental pollutants, it has been observed that exposures tend to follow an inverted-U trajectory over time as exposures rise and then fall in parallel with increasing wealth, literacy and technological development. This is sometimes referred to as the 'environmental Kuznets' curve (figure)[2]. Low income populations tend to suffer most from households exposures, such as those relating to lack of access to clean water and sanitation, and exposure to indoor pollution from the inefficient and inadequately ventilated burning of biomass fuels for domestic cooking and heating. Middle income populations on the other hand suffer more from community-level pollution, such as urban outdoor air pollution, contaminated water sources, and occupational hazards. High income populations have, for the most part, reduced these risks, but contribute disproportionately to global problems, including greenhouse gas emissions, persistent organic pollutants (POPs), ozone-depleting gases, and urban non-biodegradable waste.
|
Environmental burdens of disease
|
Global burdens of disease |
It is difficult to provide definitive estimates of the environmental burden of disease because of issues of definition, incomplete evidence about aetiology, and the complexities of assessing exposures and their longer-term effects. But estimates suggest that somewhere between a quarter and a third of the global burden of disease and premature death is attributable to direct environmental risk factors. The international Global Burden of Disease initiative has attempted to derive estimates of mortality and disability adjusted life years (DALYs) for selected causes. The mortality and DALYs attributed to childhood and maternal under-nutrition are given for comparison (table). For the environment they indicate that the largest burdens globally arise from unsafe water and sanitation and indoor smoke (both mainly affecting populations in the developing world), and outdoor air pollution (mainly affecting middle income populations, especially in Asia). The effects of global climate change are expected to grow substantially over time.
|
|||||||||||||||||||||||||||
In 2014, WHO estimate that diarrhoeal disease accounts for approximately 3.6% of the total DALY global burden of disease, and of this it is estimated that 58% is attributable to unsafe water supply, sanitation and hygiene, most of which is in developing countries (WHO 2014).
Key references
- Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002; 360(9343):1347-60 Doi:10.1016/S0140-6736(02)11403-6
- Murray et al. Global Burden of Disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020 : http://www.hup.harvard.edu/catalog.php?isbn=9780674354487
- Jones KE, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL, et al. Global trends in emerging infectious diseases. Nature. 2008 Feb 21;451(7181):990-3
- WHO. Preventing diarrhoea through better water, sanitation and hygiene. 2014: available from: http://apps.who.int/iris/bitstream/10665/150112/1/9789241564823_eng.pdf?ua=1/&ua=1
- WHO Global Burden of disease Study (2013) http://www.who.int/healthinfo/global_burden_disease/gbd/en/
- Whiteford et al. Global burde of disease attritbutable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. The Lancet. 2013
382: 9904: 1575-1596.
Useful websites
- United States Environmental Protection Agency, pages on Health Science https://www.epa.gov/science-and-technology/health-scienceUN Millennium Development Goals http://www.un.org/millenniumgoals/Preventing disease through healthy environments. WHO 2016: http://apps.who.int/iris/bitstream/10665/204585/1/9789241565196_eng.pdf?ua=1
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015; 386: 743-800.
© Dr Paul Wilkinson 2009, Rebecca Close and Helen Crabbe 2016
[3] Murry, C.J.L et al (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet , Volume 380, Issue 9859, 15 December 2012–4 January 2013, Pages 2197–2223. http://www.sciencedirect.com/science/article/pii/S0140673612616894